News
2022 Update
February 10, 2022

“There are countries where communicable and/or non-communicable diseases, pregnancy and childbirth, and injuries are still causing hundreds of thousands, and in some cases millions, of deaths among people under 50 each year.”
Leith Greenslade is the Founder and CEO of JustActions, an organization working to accelerate global progress/collaboration on a variety of fronts, including global health and innovation. Before that, she was a Vice-Chair at the MDG Health Alliance, a special initiative of the Office of the United Nations Special Envoy for Financing the Health Millennium Development Goals in support of Every Woman, Every Child, an unprecedented movement spearheaded by the United Nations Secretary-General to advance the health of women and children. Leith is a member of the Board of TEAMFund.
Larry Summers argued in “The Future of Aid for Health” that there should be a “substantial reallocation” of foreign health aid towards global public goods, such as developing medicines and vaccines for diseases of poverty; managing cross-border externalities (e.g., pandemics, antimicrobial resistance), and fostering global health leadership and stewardship, including improving priority-setting processes.
This is a good list, but the most important item is buried at the bottom – priority-setting. Without setting the right priorities about which health technologies to develop, which externalities to manage, and which leaders to steward, health impact will fall short.
Health technologies have already contributed significantly to reducing preventable deaths in many countries, but currently no country has achieved all of the Sustainable Development Goals (SDGs) for health.
While some countries are on track to do so by 2030, many will struggle. These are the countries where communicable and/or non-communicable diseases, pregnancy and childbirth, and injuries are still causing tens of thousands, and in some cases millions, of deaths among people under 50 each year.
For these countries, the strategic adoption of health technologies that target the leading causes of early death, and the associated risks for death, hold the greatest promise for SDG progress.
But what are the leading causes and risks for early death, where are the most vulnerable populations, and which health technologies could save and improve the most lives and dramatically accelerate achievement of the health SDGs?
An analysis of the latest Global Burden of Disease (GBD) data from 2019 tells an important story.
Priority causes
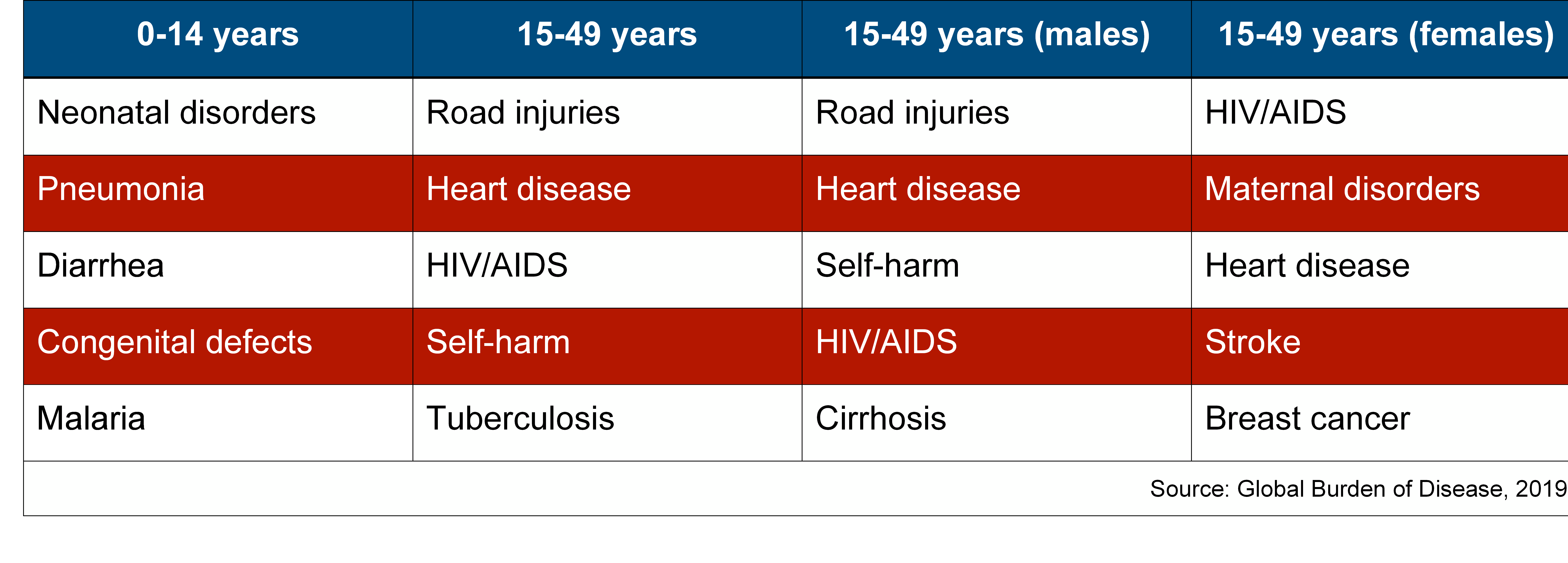
The leading causes of early death among children and working-age adults differ. Neonatal causes, principally preterm birth, birth trauma, and sepsis, infectious diseases like pneumonia, diarrhea, and malaria, and congenital birth defects, especially heart defects, are the leading causes of child death.
In contrast, the leading causes of death among working-age adults include road injuries, heart disease, HIV/AIDS, self-harm, and tuberculosis. Cirrhosis, a condition of the liver, is also a leading cause of death among young men, and maternal disorders (death during pregnancy or as a result of childbirth), breast cancer, and stroke are leading causes of death among young women (chart 1).
It is important to note that both communicable and non-communicable diseases are among the top five causes of early death for children and adults, and the increasing role that co-morbidities (the interaction between infectious and non-infectious causes of death in the same population) play in sustaining high burdens of early death.
Chart 1: Leading causes of early death (0-49 years)
 Source: Global Burden of Disease, 2019
Source: Global Burden of Disease, 2019
Priority risks
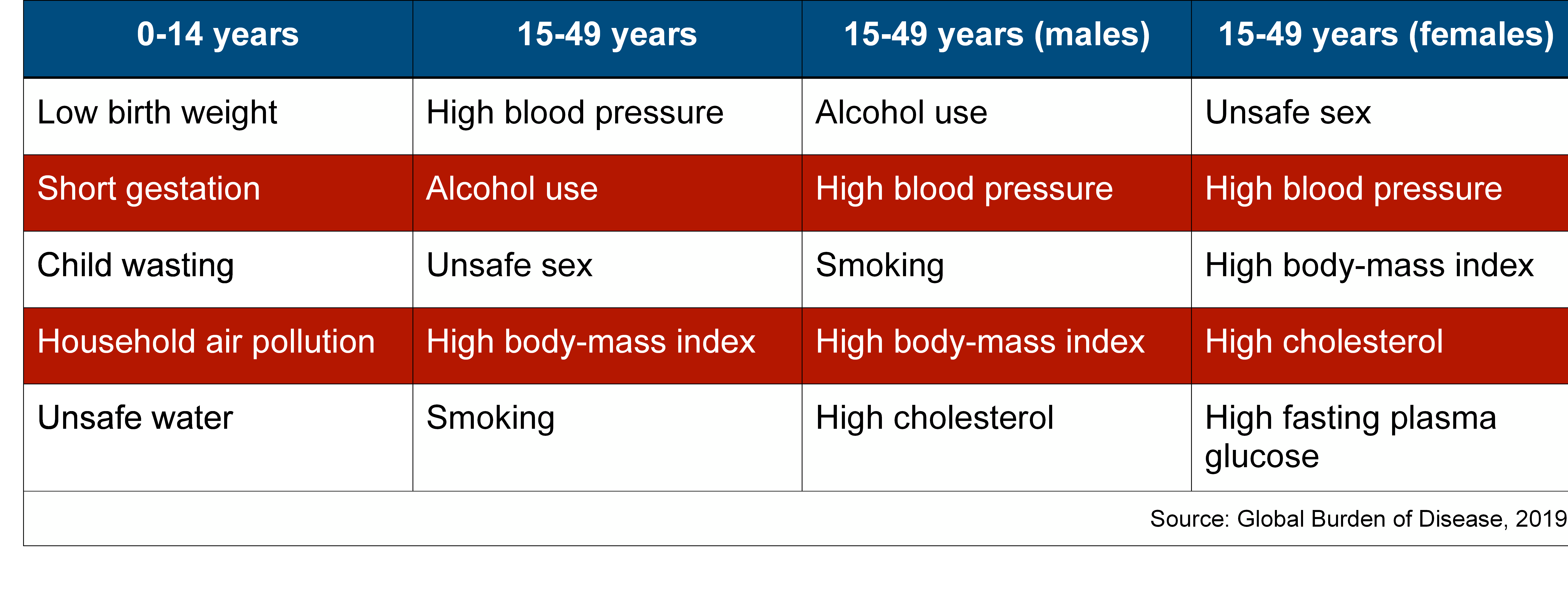
Specific factors increase the risk of early death. Among children, they include low birth weight (2,500 grams or less at birth), short gestation (<37 weeks gestation at birth), child wasting (a child who is too thin for his/her height due to recent rapid weight loss or the failure to gain weight), household air pollution (primarily from indoor cooking on open fires), and unsafe water.
Among those aged 15 to 49 years, the leading risks for early death include high blood pressure, alcohol use, unsafe sex, high body-mass index, and smoking. High cholesterol is also a major risk for both young men and women, while high fasting plasma glucose which contributes to diabetes is a specific risk for young women (chart 3).
As all of these risks relate to unhealthy behaviors - alcohol use, smoking, unsafe sex, and poor diet, health technologies that can successfully change human behavior - especially what we eat and drink - will prevent many deaths.
Chart 2: Leading risks for early death (0-49 years)
 Source: Global Burden of Disease, 2019
Source: Global Burden of Disease, 2019
Priority populations
In 2019, there were 13 million deaths among people under 50 years of age - 23% of all deaths - with 70% clustered in just 20 countries (chart 3).

India is the clear outlier, with 2.6 million early deaths, but Nigeria and China are also each losing more than 1 million children and working-age adults every year. And Pakistan, Indonesia, the Democratic Republic of Congo (DRC), Ethiopia, Brazil, the USA, and Russia are each losing more than 200,000 children and working-age adults each year.
In some of these countries, early deaths cluster among children (Nigeria, DRC, Ethiopia, Tanzania, Uganda, Afghanistan, and Mali), while in others deaths cluster among working-age adults (China, Brazil, USA, Russia, South Africa, and Mexico). And some countries are dealing with heavy burdens of early death among both populations, including India, Pakistan, Indonesia, Bangladesh, the Philippines, Mozambique, and Kenya.
Early deaths as a percentage of all deaths in the 20 countries range from a low 9% in the USA to a high of 72% in Mali. Most of the countries where more than 50% of all early deaths occur are in Sub-Saharan Africa. In contrast, the countries where less than 20% of deaths are early are all in Asia, Europe, and North America.
The rate of progress in reducing early deaths also differs markedly across the 20 countries. Between 2000 and 2019, eight countries reduced early deaths by more than 25% (India, China, DRC, Ethiopia, Russia, South Africa, Bangladesh, and Uganda), while Pakistan, the Philippines and Afghanistan recorded rates below 10%. Of concern, early deaths actually increased in three of the countries over the period, including in the USA, Mexico, and Mali.
Priority health investments
Technologies that target the leading causes of early death in the largest populations at greatest risk will have the greatest impact on population health and the achievement of the health SDGs.
This means that technologies that can prevent, diagnose, and/or treat the leading causes of early death and reduce the leading risk factors among children, young women, and young men in the 20 countries that lose the most young people should be prioritized.
In most countries, this will require investing in the development and uptake of health technologies that target three key areas:
Technologies that reduce the underlying risk factors associated with early death would include tools that can lower rates of low birth weight, short gestation, and wasting, and improve access to clean water and air for children. Among working-age adults the investments that could save the most lives will be able to cost-effectively reduce alcohol use, high blood pressure, and smoking among young men, and unsafe sex, high blood pressure, and high body-mass index and among young women.
Child health priorities
For the countries where early deaths are concentrated among children, investments in new tools that prevent preterm birth and congenital birth defects, diagnose women at risk early in pregnancy, make childbirth safer, and effectively treat babies born with complications are urgent priorities. In fact, an entire suite of products is needed to retool Neonatal Intensive Care Units (NICUs) in low-resource settings.
Technologies that improve the prevention, diagnosis, and treatment of child pneumonia, diarrhea, and malaria will also save many lives and are the most important infectious disease priorities for children. The holy grail is a rapid diagnostic test that can distinguish viral pneumonia from bacterial pneumonia and malaria at the point of care. As malnutrition is driving more than a half of all child deaths, investments that can prevent child wasting by improving access to breastmilk (e.g., via human milk banks), and/or improve the effectiveness of wasting treatments will substantially reduce the risk of child death.
Men’s health priorities
To reduce deaths among working-age men, health technologies that can prevent, diagnose, and/or treat heart disease and cirrhosis will have a major and growing impact, as deaths from non-communicable diseases continue to rise in the 20 countries. However, in many of the 20 countries, investments that target the leading communicable killers, especially HIV/AIDS, will remain critical until the spread of infections has been controlled. And as self-harm is a leading killer of young men, technologies that improve mental health and reduce the risk of suicide will also have a major impact.
To reduce the risk of death among young men, new tools that target high blood pressure, high body mass index, and high cholesterol will have a major impact on reducing non-communicable disease deaths, while technologies that reduce alcohol and smoking will benefit all-cause early mortality among working-age men.
Women’s health priorities
Among working-age women, the clear investment priorities are new tools with the power to reduce deaths from HIV/AIDS, maternal disorders, heart disease, stroke, and breast cancer, in that order. Investments that reduce the risk of death in pregnancy and childbirth are especially critical in a subset of African and Asian countries, as well as technologies that can prevent the spread of HIV/AIDS. New diagnostic tools that include the major infectious diseases and chronic conditions that threaten healthy pregnancies are desperately needed and could save many lives in these settings.
Investments that reduce the risks of unsafe sex and unplanned pregnancies (e.g., long-lasting, self-administered contraceptives) among young women will have an outsize impact on lives saved as this is the leading risk factor for early death among women. New tools that reduce the risks of high blood pressure, high body-mass index, high cholesterol, and high fasting plasma glucose will have a major impact on reducing early deaths from non-communicable diseases, such as heart disease, stroke, and diabetes.
Priority channels
How these solutions are developed, financed, and ultimately made available in the target populations matters. Innovations that emerge from their country contexts or that are sourced elsewhere and adapted by local institutions, often in partnership with external stakeholders, stand the best chance of success. As private financing for development now dwarfs foreign aid by more than eight to one, investments that crowd in private capital to finance both health innovations and access to them will have the greatest potential for impact. For these investments, success will be measured in the scale of lives saved and sickness averted, and in the way they lay a solid foundation for local pro-health markets to develop.
For those countries where most healthcare is provided by the private sector, investments in companies will yield the highest impact returns. Where private investment dollars – offered as loans, subsidies, guarantees, grants and/or equity – find their way to companies that pursue shared value strategies, and/or to local start-up social businesses, they have the potential to leave a lasting legacy of better health for future generations. These will be the type of companies that build products to serve one or more of the leading causes and/or risks of early death in one or more of the 20 countries presented in this analysis.
Companies with a CEO and management team deeply committed to health impact, and who are as comfortable with public health data as they are with profit and loss statements will have an impact edge. Teams with the ability to craft business strategies that serve both the bottom line and the SDGs, and the skills to work “across the aisles” with governments, universities, and non-profits will represent competitive impact investment opportunities.
For the countries where most healthcare for the vulnerable is provide by governments and/or non-profit services, investors will need to find efficient and effective ways to invest directly in government services (e.g., fee for service) and/or to support non-profit services (e.g., grants), being careful not to displace public sector funding for health or to divert talent.
Irrespective of the mode of delivery – public or private sector – the most successful investments across the 20 countries will be those with a technology or service that passes the price/performance tradeoff, either by offering the same solution at a lower cost, by offering a new solution at the same cost, or by offering a new solution that performs better at lower cost (the best investment proposition of all).
Investors that are seeking health impact in Asia should therefore be supporting governments, companies, and/or non-profits to reduce neonatal deaths and child deaths from pneumonia, diarrhea, and congenital defects, and the major risk factors - low birth weight, short gestation wasting, and air pollution. Among young adults, new technologies that reduce deaths from heart disease, stroke, cirrhosis, and tuberculosis will have the greatest health impact, together with risk reduction tools that target smoking, alcohol use, high blood pressure, high body-mass index and high cholesterol. Investments in India, China, Pakistan, Indonesia, Bangladesh, the Philippines and/or Afghanistan will have the highest health impact.
Investors seeking health impact in Africa should support efforts in Nigeria, DRC, Ethiopia, South Africa, Mali, Tanzania, Mozambique, Uganda, Kenya and/or Mali to reduce neonatal and maternal deaths, and/or child deaths from pneumonia, diarrhea, and/or malaria. Investments that target the leading risk factors of low birth weight, short gestation, wasting, unsafe water, and household air pollution will also yield major health benefits. With respect to working-age adults, organizations with technologies that can reduce rates of HIV/AIDS, tuberculosis, malaria, and heart disease - as well as reduce the risks of unsafe sex, alcohol use, and air pollution, high blood pressure, and high body-mass index - should be investment priorities.
It is important to note that investors can still make a major impact on health and the SDGs by investing in the large, underserved populations in Brazil, the USA, Russia, and Mexico where heart disease, cirrhosis, HIV/AIDS, stroke, and chronic kidney disease dominate among causes of early death. Technologies that target these causes as well as the major risk factors for early death in these countries – alcohol use, high body-mass index, smoking, high blood pressure, and high fasting plasma glucose – will deliver major health gains. Investments in governments, companies, and/or non-profits that reach the underserved populations of these four higher income countries do represent high impact health investments in the context of the SDGs.
In summary, the path to global health impact for investors begins with setting the right priorities. By identifying the largest populations most vulnerable to early death and the leading causes and risks of death, and then investing in the most cost-effective technologies that target these causes and risks in these populations, investors can maximize their impact on health and the SDGs.
In countries where the vast majority of health services are delivered by the private sector, investments in companies and social businesses will be essential, while in the countries where governments and/or non-profit organizations dominate health provision, investments in the public and non-profit sector actors will offer the most direct path to impact.